Imagine a guided missile that can precisely target cancer cells while leaving healthy ones relatively unharmed. That’s the basic idea behind antibody drug conjugates, or ADCs. These fascinating molecules are becoming a major force in medicine, particularly in the fight against cancer, and it’s a field that’s rapidly evolving.
The market for ADCs is buzzing. What started as a niche area is now a multi-billion-dollar industry, and it’s only expected to grow. Why? Because ADCs are showing real promise in treating various cancers, from breast cancer and lymphoma to leukemia. The ability to deliver powerful chemotherapy directly into cancer cells, minimizing the nasty side effects that traditional chemo can cause, is a game-changer.
Table of contents
- What are antibody drug conjugates (ADC)?
- ADC therapy components
- How do ADCs work?
- Tools for ADC development and manufacturing
- What’s next for ADCs
- More resources
What are antibody drug conjugates (ADC)?
An antibody-drug conjugate (ADC) is a targeted cancer therapy that combines the specificity of monoclonal antibodies with the potency of cytotoxic drugs. This approach allows for the direct delivery of chemotherapy agents to cancer cells, minimizing damage to healthy tissues.
Science in analogy: ADCs as “smart bombs” against disease targets
Scientifically, ADCs are a clever combination of different concepts in biologic therapeutics.
First is the antibody, which is like a homing device that specifically recognizes antigen markers on cancer cells or other disease targets. Then you have a potent drug as the “warhead” designed to kill those cells. The crucial molecular link between the two is known as the linker.
Scientists are constantly working on better antibodies that are even more specific to cancer, developing more powerful and targeted drugs, and creating linkers that are stable in the bloodstream but release their payload once they reach the tumor. We’re seeing new approaches like using bispecific antibodies that can target multiple markers on a cancer cell or antibodies carrying different types of drugs, like those that can boost the patient’s own immune system.
ADC therapy components
Structurally, an ADC comprises three components: a monoclonal antibody that binds to a tumor-associated antigen, a cytotoxic payload, and a chemical linker that connects the two. The antibody targets antigens overexpressed on cancer cells, ensuring selective delivery.
Monoclonal antibody (mAb)
The monoclonal antibody serves as the targeting moiety, engineered to recognize and bind specific antigens that are overexpressed on tumor cells but minimally present on normal tissues. This specificity facilitates selective delivery of the cytotoxic payload to malignant cells, enhancing therapeutic efficacy while reducing systemic toxicity.
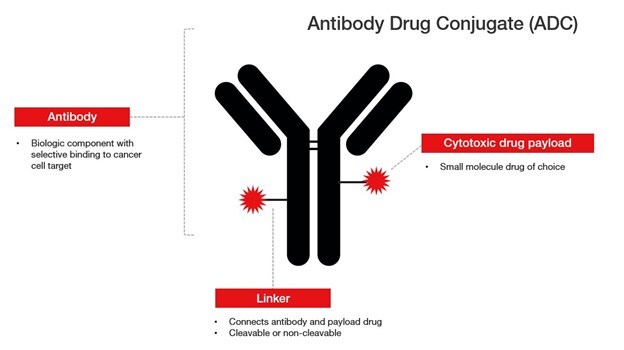
Linker
The linker is a chemical bridge that connects the mAb to the cytotoxic payload. It must be stable in the bloodstream to prevent premature release of the drug, yet cleavable within the target cell to ensure effective payload delivery. Linkers are categorized as cleavable or non-cleavable. Cleavable linkers exploit intracellular conditions—such as acidic pH or specific enzymes like cathepsins—to release the payload, while non-cleavable linkers rely on complete degradation of the antibody within the lysosome to liberate the active drug.
Cytotoxic payload
The cytotoxic payload is a highly potent small-molecule drug designed to kill cancer cells upon internalization. Common payloads include microtubule inhibitors (e.g., monomethyl auristatin E) and DNA-damaging agents (e.g., calicheamicin). Due to their high toxicity, these agents are unsuitable for systemic administration but are effective when selectively delivered via ADCs.
Dual payload ADCs
An emerging advancement in ADC technology is the development of dual-payload ADCs, which incorporate two distinct cytotoxic agents within a single conjugate. This strategy aims to address tumor heterogeneity and drug resistance by simultaneously targeting multiple cellular pathways. Dual-payload ADCs can be designed to deliver drugs with complementary mechanisms of action, potentially enhancing antitumor activity and overcoming resistance to single-agent therapies.
How do ADCs work?
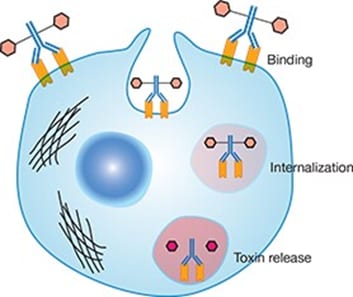
Upon binding to its target antigen, the ADC is internalized into the cancer cell via receptor-mediated endocytosis. The internalized complex is trafficked to lysosomes, where the linker is cleaved, releasing the cytotoxic drug.
Within the lysosome, the linker plays a pivotal role in controlling the release of the cytotoxic payload. Linkers are designed to be stable in circulation but cleavable within the intracellular environment, often exploiting the acidic pH or specific lysosomal enzymes. For instance, peptide-based linkers sensitive to cathepsin B are commonly employed, ensuring that the cytotoxic agent is liberated predominantly within the target cell’s lysosome.
Once released, the cytotoxic payload disrupts critical cellular processes, such as DNA replication or microtubule function, leading to cancer cell death. Some ADCs also exhibit a “bystander effect,” where the released drug diffuses into neighboring tumor cells, including those lacking the target antigen. This bystander phenomenon is particularly beneficial in treating heterogeneous tumors where not all cells express the target antigen uniformly.
The clinical success of ADCs depends on the careful optimization of each component—antibody specificity, linker stability and cleavability, and payload potency. Advancements in linker technology, such as dual-enzyme cleavable linkers, have further refined the specificity and efficacy of ADCs.
Mechanism of Action At-a-Glance
- Target binding: The monoclonal antibody component of the ADC specifically binds to an antigen expressed on the surface of cancer cells.
- Internalization: Upon binding, the ADC-antigen complex is internalized into the cancer cell through endocytosis.
- Drug release: Inside the cell, the linker connecting the antibody to the cytotoxic drug is cleaved, often within the lysosomal compartment, releasing the active drug.
- Cell death: The released cytotoxic agent interferes with critical cellular processes, such as DNA replication or microtubule function, leading to cancer cell death.
Tools for ADC development and manufacturing
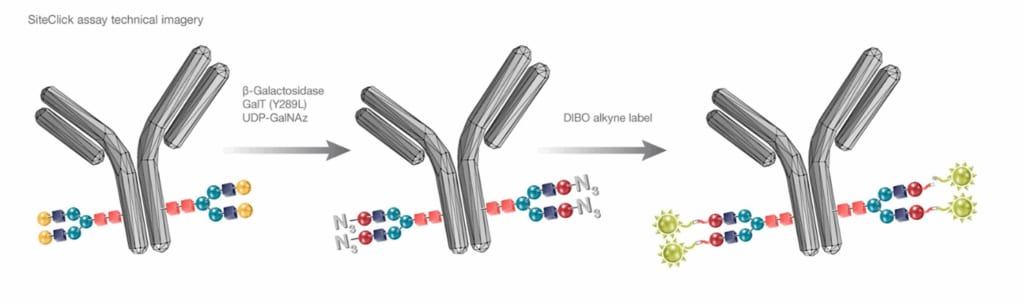
At Thermo Fisher Scientific, we offer a wide range of tools and technologies that help researchers and manufacturers develop and produce ADCs more efficiently and safely. This includes everything from cell culture systems like the Gibco™ ExpiCHO™ Expression System for producing antibodies to antibody conjugation tools like Invitrogen™ SiteClick™ Antibody Labeling Kits or our custom recombinant antibody services.
Tools for optimizing ADC workflow
- Gene synthesis and high-throughput antibody expression: GeneArt HTP Antibody Expression Service, a semi-automated, high-throughput platform enabling reproducible and rapid production of antibodies from transiently transfected mammalian cells
- Expression and purification: ExpiCHO Expression System to achieve transient expression yields of 1-3 g/L for antibody and non-antibody proteins; Nalgene 5L Angled Flask
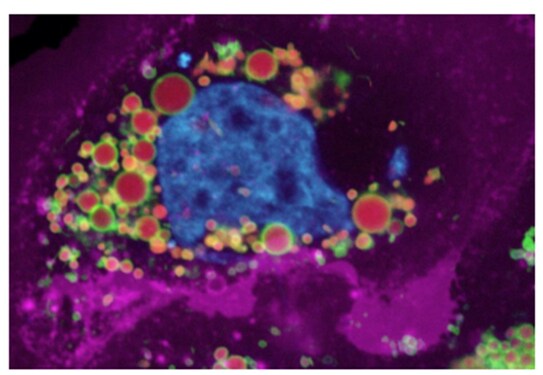
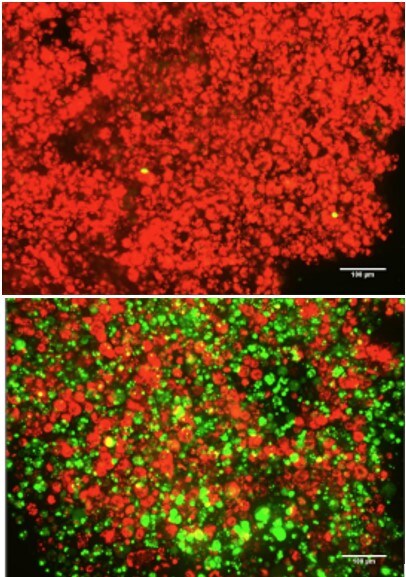
- Antibody labeling: SiteClick or LysoLight labelling kits for specific and sensitive detection of internalized antibodies within lysosomes using fluorescence microscopy, flow cytometry, or high content imaging platforms
- Imaging and high-content analysis: EVOS M7000 Imaging System, CellInsight CX7 LZR Pro High Content Screening Platform
FDA approved ADC drugs
As of May 2025, the FDA has approved 15 ADC drugs for clinical use. More than a hundred ADC candidates are also in the clinical pipeline for evaluation.
| Drug | Approval year | Payload | Target | Disease Indication |
|---|---|---|---|---|
| Gemtuzumab Ozogamicin (Mylotarg) | 2000*, 2017 | Calicheamicin | CD33 | Acute myelogenous leukemia (AML) |
| Brentuximab Vedotin (Adcetris) | 2011 | MMAE | CD30 | Hodgkin lymphoma (HL), anaplastic large cell lymphoma (ALCL) |
| Trastuzumab Emtansine (Kadcyla) | 2013 | DM1 | HER2 | Breast cancer |
| Inotuzumab Ozogamicin (Besponsa) | 2017 | Calicheamicin | CD22 | Acute lymphoblastic leukemia (ALL) |
| Moxetumomab Pasudotox (Lumoxiti) | 2018* | PE38 | CD22 | Hairy cell leukemia (HCL) |
| Polatuzumab Vedotin (Polivy) | 2019 | MMAE | CD79b | Diffuse large b-cell lymphoma (DLBCL) |
| Enfortumab Vedotin (Padcev) | 2019 | MMAE | Nectin-4 | Urothelial (bladder) cancer |
| Trastuzumab Deruxtecan (Enhertu) | 2019 | DXD | HER2 | Breast cancer |
| Belantamab mafodotin-blmf (Blenrep) | 2020* | MMAF | BCMA | Multiple myeloma |
| Sacituzumab Govitecan (Trodelvy) | 2020 | SN-38 | TROP2 | Breast cancer, urothelial (bladder) cancer |
| Disitamab Vedotin (Aidixi) | 2021 | MMAE | HER2 | Gastric cancer, urothelial (bladder) cancer |
| Loncastuximab Tesirine (Zynlonta) | 2021 | PBD SG3199 | CD19 | Diffuse large b-cell lymphoma (DLBCL) |
| Tisotumab Vedotin (Tivdak) | 2021 | MMAE | TF | Cervical cancer |
| Mirvetuximab Soravtansine (Elahere) | 2022 | DM4 | FRα | Ovarian cancer |
| Datopotamab Deruxtecan (Datroway) | 2025 | DXD | TROP-2 | HR+/HER2– breast cancer |
| Telisotuzumab vedotin (Emrelis) | 2025 | MMAE | c-Met | non-small cell lung cancer (NSCLC) |
*Product withdrawn or discontinued from market
Regulatory landscape in 2025
The FDA has classified ADCs as combination products, comprising both a biological product (the antibody) and a drug (the cytotoxic payload). This classification requires adherence to regulatory requirements pertinent to both biologics and small-molecule drugs, impacting manufacturing practices, quality control, and approval pathways.
In April 2025, the FDA announced a strategic initiative to phase out traditional animal testing in drug development, including for ADCs. The agency is encouraging the adoption of New Approach Methodologies (NAMs), such as artificial intelligence-based models and laboratory-engineered human organ-like structures, to enhance drug safety assessments and reduce reliance on animal models.
The FDA has also at times provided expedited routes to ADC therapy approvals. For instance, in May 2025, the agency granted accelerated approval to Emrelis (telisotuzumab vedotin) for the treatment of adults with previously treated non-squamous non-small cell lung cancer (NSCLC) exhibiting high c-Met protein overexpression.
What’s next for ADCs
Looking to the future, the field of ADCs is incredibly exciting. We’re likely to see even more precise targeting strategies, perhaps using smaller targeting molecules derived of antibody fragments or cell surface receptor binding moieties or going after novel markers on cancer cells. Scientists are also working on “smarter” linkers that release their payload more specifically within the tumor environment. Combination therapies, where ADCs are used alongside other cancer treatments like immunotherapy, are also showing great promise. Beyond cancer, researchers are exploring the potential of ADCs to treat other diseases, such as autoimmune disorders and even infections.
In short, antibody-drug conjugates represent a powerful and evolving approach to targeted therapy. While there are challenges in their development and production, the scientific progress and the dedication of companies providing innovative solutions are paving the way for a future where these “smart bombs” can offer more effective and less toxic treatments for a wide range of diseases.
More resources
- Handbook: Antibody drug conjugate screening and characterization
- Tools: Antibody internalization and degradation assays for ADC discovery
- Tools: Improved labeling tools for ADC screening and characterization
- Poster: Modular, defined assembly of antibody-based constructs using click chemistry
- App Note: Antibody–drug conjugate development: from antibody production to characterization
##
© 2025 Thermo Fisher Scientific Inc. All rights reserved. All trademarks are the property of Thermo Fisher Scientific and its subsidiaries unless otherwise specified.
For Research Use Only. Not for use in diagnostic procedures.

Raw material considerations for cell therapy manufacturing
In cell therapy manufacturing, the lack of definitive regula... Tanuka Biswas, PhD
Read More
Scale-Up vs. Scale-Out Strategies for Continuous Pharma Manufacturing
As pharmaceutical pipelines evolve, manufacturing strategies... Dirk Leister
Read More
Cryopreservation: Advancements in Human Stem Cell-Derived Neurons
The field of cryopreservation has seen advancements, particu...
Read More
Multiplex vs. Singleplex qPCR: What do I need to know?
Real-time PCR (qPCR) has transformed how scientists detect a... John Pfeifer, PhD
Read More
Leave a Reply