Search
Zeta
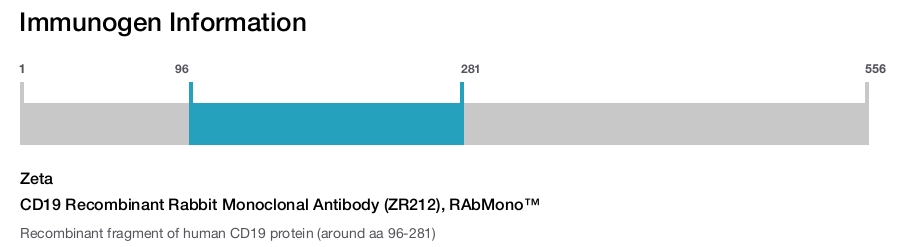
CD19 Recombinant Rabbit Monoclonal Antibody (ZR212), RAbMono™
{{$productOrderCtrl.translations['antibody.pdp.commerceCard.promotion.promotions']}}
{{$productOrderCtrl.translations['antibody.pdp.commerceCard.promotion.viewpromo']}}
{{$productOrderCtrl.translations['antibody.pdp.commerceCard.promotion.promocode']}}: {{promo.promoCode}} {{promo.promoTitle}} {{promo.promoDescription}}. {{$productOrderCtrl.translations['antibody.pdp.commerceCard.promotion.learnmore']}}
Additional Information:
{{banner.description}}
 (IHC (P))")
 in IHC (P)")
产品信息
Z2547RS
产品规格
种属反应
Human
宿主/亚型
Rabbit
/ IgG
Expression System
CHO cells
分类
Recombinant Monoclonal
类型
Antibody
克隆号
ZR212
抗原
Recombinant fragment of human CD19 protein (around aa 96-281)
偶联物
Unconjugated
Unconjugated
Unconjugated
形式
Liquid
浓度
200 µg/mL
规格
100 µg
纯化类型
Protein A
保存液
tris with BSA, NP-40
内含物
<0.1% sodium azide
保存条件
4°C
运输条件
Ambient (domestic); Wet ice (international)
产品详细信息
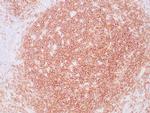
A recommended positive control tissue for this product is Lymph Node, however positive controls are not limited to this tissue type.
The primary antibody is intended for laboratory professional use in the detection of the corresponding protein in formalin-fixed, paraffin-embedded tissue stained in manual qualitative immunohistochemistry (IHC) testing. This antibody is intended to be used after the primary diagnosis of tumor has been made by conventional histopathology using non-immunological histochemical stains.
In normal lymphoid tissue CD19 is observed in germinal centers (on both B cells and follicular dendritic cells), in mantle zone cells and in scattered cells in the interfollicular areas, with an overall immunoreactivity pattern similar to that of CD20 and CD22. However, in contrast to CD20, CD19 is also expressed in pre-B cells. CD19 positivity is seen in the vast majority of B-cell neoplasms (B-lymphoblastic lymphoma, small lymphocytic lymphoma/CLL, mantle cell lymphoma, follicular lymphoma, Burkitt lymphoma, marginal zone lymphoma, diffuse large B-cell lymphoma, T-cell-rich B-cell lymphoma, lymphoblastic lymphoma, hairy cell leukemia) and commonly at a lower intensity than normal B-cell elements. Plasma cell neoplasms are consistently negative as are T-cell neoplasms. CD19 was undetectable in 14% of diffuse large B-cell lymphomas, 30% of T-cell-rich B-cell lymphomas and 75% of post-transplant B-lymphoproliferative disease. CD19 expression is not seen in Reed Sternberg cells of classic Hodgkin lymphoma.
Antibody is used with formalin-fixed and paraffin-embedded sections. Pretreatment of deparaffinized tissue with heat-induced epitope retrieval or enzymatic retrieval is recommended. In general, immunohistochemical (IHC) staining techniques allow for the visualization of antigens via the sequential application of a specific antibody to the antigen (primary antibody), a secondary antibody to the primary antibody (link antibody), an enzyme complex and a chromogenic substrate with interposed washing steps. The enzymatic activation of the chromogen results in a visible reaction product at the antigen site. Results are interpreted using a light microscope and aid in the differential diagnosis of pathophysiological processes, which may or may not be associated with a particular antigen.
A positive tissue control must be run with every staining procedure performed. This tissue may contain both positive and negative staining cells or tissue components and serve as both the positive and negative control tissue. External Positive control materials should be fresh autopsy/biopsy/surgical specimens fixed, processed and embedded as soon as possible in the same manner as the patient sample (s). Positive tissue controls are indicative of correctly prepared tissues and proper staining methods. The tissues used for the external positive control materials should be selected from the patient specimens with well-characterized low levels of the positive target activity that gives weak positive staining. The low level of positivity for external positive controls is designed to ensure detection of subtle changes in the primary antibody sensitivity from instability or problems with the staining methodology. A tissue with weak positive staining is more suitable for optimal quality control and for detecting minor levels of reagent degradation.
Internal or external negative control tissue may be used depending on the guidelines and policies that govern the organization to which the end user belongs to. The variety of cell types present in many tissue sections offers internal negative control sites, but this should be verified by the user. The components that do not stain should demonstrate the absence of specific staining, and provide an indication of non-specific background staining. If specific staining occurs in the negative tissue control sites, results with the patient specimens must be considered invalid.
靶标信息
CD19 is a member of the immunoglobulin superfamily, characterized by two Ig-like domains, and is expressed on B cells throughout all stages of development, excluding terminally differentiated plasma cells. It is also expressed on follicular dendritic cells and has been observed on myeloid leukemia cells, particularly those of monocytic lineage. CD19 is considered the earliest and broadest B cell-restricted antigen, and its expression is found in all B cell precursor leukemias. CD19 forms a multimolecular complex with CD21, CD81, Leu13, MHC class II, and the B cell receptor (BCR), playing a crucial role in B cell signaling. As a signal-amplifying coreceptor for the BCR, CD19 lowers the threshold for antigen receptor-dependent stimulation, allowing B cells to respond specifically and sensitively to various antigens through low-affinity antigen receptors. Signaling through CD19 induces tyrosine phosphorylation, calcium flux, and proliferation of B cells. Beyond its role as a BCR coreceptor, CD19 can also signal independently of BCR co-ligation, serving as a central regulatory component upon which multiple signaling pathways converge. This makes CD19 an important functional regulator of both normal and malignant B cell proliferation. Mutations in the CD19 gene can result in hypogammaglobulinemia, a condition characterized by low levels of immunoglobulins, while CD19 overexpression can lead to B cell hyperactivity. CD19 is expressed on 100% of peripheral B cells, as defined by the expression of kappa or lambda light chains, underscoring its significance in B cell function and immune regulation.
仅用于科研。不用于诊断过程。未经明确授权不得转售。
篇参考文献 (0)
您是否在文献中引用过该产品?请点击下方按钮邮件告知我们。
生物信息学
蛋白别名: B-lymphocyte antigen CD19; B-lymphocyte surface antigen B4; CD19; CD19 differentiation antigen; Differentiation antigen CD19; Leu-12; T-cell surface antigen Leu-12; unnamed protein product
基因别名: B4; CD19; CVID3
UniProt ID: (Human) P15391
Entrez Gene ID: (Human) 930
B-1 B cell differentiation
adaptive immune response
B cell proliferation involved in immune response
immune system process
immunoglobulin mediated immune response
B cell mediated immunity
B cell proliferation
antigen receptor-mediated signaling pathway
B cell receptor signaling pathway
regulation of B cell receptor signaling pathway
regulation of B cell activation
positive regulation of release of sequestered calcium ion into cytosol
positive regulation of protein kinase B signaling
Disclaimer

Clicking the images or links will redirect you to a website hosted by BenchSci that provides third-party scientific content. Neither the content nor the BenchSci technology and processes for selection have been evaluated by us; we are providing them as-is and without warranty of any kind, including for use or application of the Thermo Fisher Scientific products presented.

